Post COVID-19 Longterm Complications;
The world’s medical and scientific communities are now facing an ever-increasing list of symptoms, in early 2020.
- no one knows how far into the future symptoms will endure, and
- whether COVID-19 will spur the onset of chronic diseases.
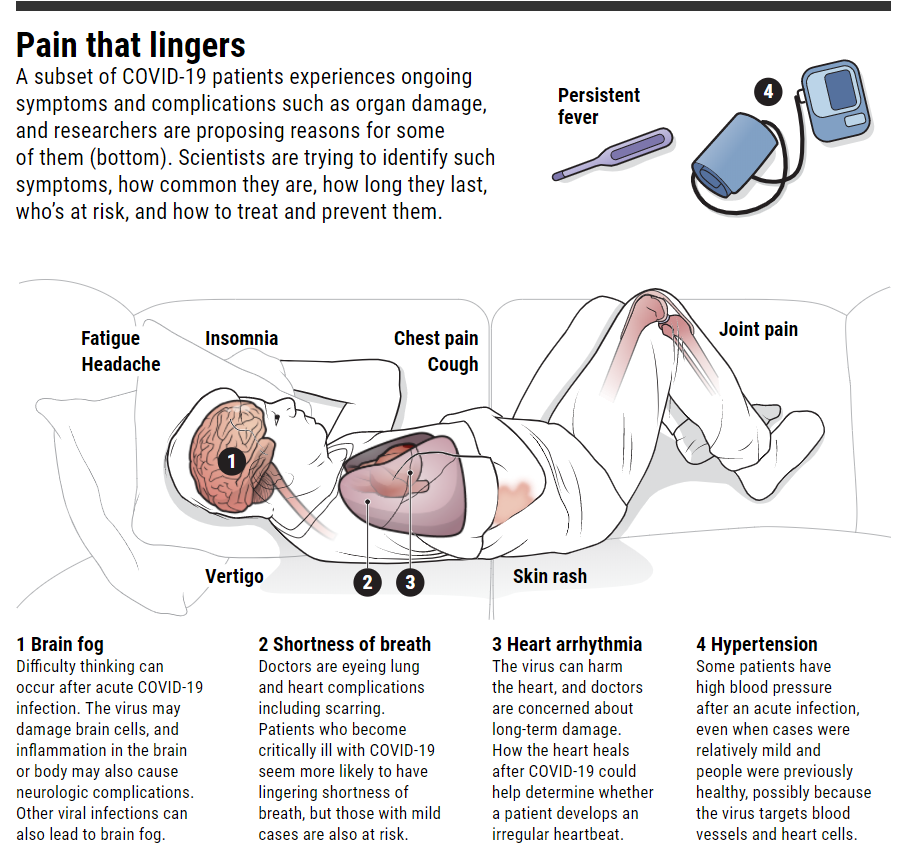
- Ongoing problems include
- fatigue,
- a racing heartbeat,
- shortness of breath,
- achy joints,
- foggy thinking,
- a persistent loss of sense of smell, and
- damage to the heart, lungs, kidneys, and brain.
Long after the fire of a Covid-19 infection, mental and neurological effects can still smolder[1]
- Beyond the fatigue, neuropsychological problems range from headaches,
- dizziness, and
- lingering loss of smell or taste to mood disorders and deeper cognitive impairment.
Doctors have concerns that patients may also suffer lasting damage to their
- heart, kidneys, and liver from the inflammation and blood clotting the disease causes.
- Additionally, between 30% and 50% of people with an infection that has clinical manifestations are going to have some form of mental health issues,” said Teodor Postolache, professor of psychiatry at the University of Maryland School of Medicine.
So far the virus appears to cause its damage to the brain and nervous system not as much through direct infection as through the indirect effects of inflammation, said Victoria Pelak, professor of neurology and ophthalmology at the University of Colorado School of Medicine.
“Strokes are larger, potentially more damaging with this disorder. Once inflammation or blood vessel problems occur within the nervous system itself, those people will have a lot longer road to recovery or may die from those illnesses,” Colorado’s Pelak said.
Doctors are also watching for a syndrome called demyelination, as in the autoimmune disease multiple sclerosis, which can cause weakness, numbness, and tingling. It can also disrupt how people think, in some cases spurring psychosis and hallucinations. “We’re just not sure if this virus causes it more commonly than other viruses,” Pelak said.
The COVID-19 infection might also act as a “priming event” for problems to resurface in the future said Teodor Postolache. Psychological stress could reactivate behavioral and emotional problems that were initially triggered by the immune system responding to the virus. “What we call psychological versus biological may actually be quite biological,” he said.
Ely of Vanderbilt suggests three things to do now.
- “We can open the hospitals back up to the families. That’s important,” he said.
- “We can be aware of these problems and tell the families about them so that the families will know that this is coming. [And]
- we can do counseling and psychological help on the back end.”
8/12/2020, MIT Technology Review:[2] Covid-19 “long haulers” are organizing online to study themselves.
Slack groups and social media are connecting people who have never fully recovered from coronavirus to collect data on their condition.
Gina Assaf was running in Washington, DC, on March 19 when she suddenly couldn’t take another step. “I was so out of breath I had to stop,” she says. Five days earlier, she’d hung out with a friend; within days, that friend and their partner had started showing three classic signs of COVID-19: fever, cough, and shortness of breath.
Assaf had those symptoms too, but a full month after falling ill, she attempted to go grocery shopping and ended up in bed for days. In those first few months, Assaf found a legion of people in situations similar to her own in a Slack support group for COVID-19 patients, including hundreds who self-identified as “long-haulers,” the term most commonly used to describe those who remain sick long after being infected.
It wasn’t until late July that the US Centers for Disease Control published a paper recognizing that as many as one-third of coronavirus patients not sick enough to be admitted to the hospital don’t fully recover. So Assaf, a technology design consultant, launched Patient-Led Research for Covid-19[ii], and released its first report[iii].
The Body Politic COVID-19 Support Group[iv]
- The Slack support group for COVID-19 patients, including hundreds who self-identified as “long-haulers,”[3] is the term most commonly used to describe those who remain sick long after being infected. In May, this group, which now calls itself Patient-Led Research for Covid-19,[4] released its first report[5].
- Based on 640 responses, it provides perhaps the most in-depth look at long-haulers to date and offers a window into what life is like for certain coronavirus patients who are taking longer—much longer—to recover.
- ‘Long-Haulers[6]’, from their first report[7] identified COVID-19 hospitalization highlights:
- Confusion[8],
- Behavior Changes[9]
- Deeper cognitive impairment
- Delirium[10]
- Exhausted/fatigue[11]
- Fumbling for words, or
- Headache[12]
- Ill-defined as “COVID fog”
- Intense stress and prolonged stress[13]
- Laid low by depression, anxiety, or PTSD[14].
- Lingering loss of smell or taste[15]
- Loss of consciousness[16]
- Mood disorders and [17]
- Peripheral nerve issues, such as Guillain-Barré syndrome, can lead to paralysis and respiratory failure[18]
- Persistent dizziness[19]
- Seizures[20]
- Stroke[21]
- They’re unable to carry on with their lives,
- Tremors
On 8/12/2020, Wes Ely, a pulmonologist and critical care physician at Vanderbilt University Medical Center who studies delirium during intensive care (watch video)[22] stay. “The problem for these people (when coming off ventilators), is not over when they leave the hospital.”
Long-term effects are health issues that are caused by an illness, disease, or treatment that lasts for several months or years after infection. Long-term effects can be physical, mental, or emotional and can occur even if the initial illness or disease is no longer present in the body.[23].
This applies to post-COVID-19 patients (Long-Haulers), as physicians and scientists from around the globe begin to study these patients post-hospitalization.

The long haul | Science science.sciencemag.org Screenshot
Also found in my LinkedIn: Compassionate Relief – COVID-19 Emerging Long-Term Complications
[1] https://www.statnews.com/2020/08/12/after-covid19-mental-neurological-effects-smolder/
[2] https://www.technologyreview.com/2020/08/12/1006602/covid-19-long-haulers-are-organizing-online-to-study-themselves/
[3] https://docs.google.com/forms/d/e/1FAIpQLScM2EeJhgisTUdo5Op6euyx1PYu8O-aNeDVYhXuPFa_Gs9PnQ/viewform
[4] https://patientresearchcovid19.com/
[5] https://docs.google.com/document/d/1KmLkOArlJem-PArnBMbSp-S_E3OozD47UzvRG4qM5Yk/edit
[6] https://docs.google.com/document/d/1KmLkOArlJem-PArnBMbSp-S_E3OozD47UzvRG4qM5Yk/edit
[7] https://docs.google.com/document/d/1KmLkOArlJem-PArnBMbSp-S_E3OozD47UzvRG4qM5Yk/edit
[8] https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/how-does-coronavirus-affect-the-brain
[9] https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/how-does-coronavirus-affect-the-brain
[10] https://www.medpagetoday.com/neurology/dementia/87543
[11] https://health.ucdavis.edu/health-news/newsroom/covid-fatigue-is-hitting-hard-fighting-it-is-hard-too-says-uc-davis-health-psychologist/2020/07
[12] https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/how-does-coronavirus-affect-the-brain
[13] https://health.ucdavis.edu/health-news/newsroom/covid-fatigue-is-hitting-hard-fighting-it-is-hard-too-says-uc-davis-health-psychologist/2020/07
[14] https://www.ptsd.va.gov/covid/COVID_effects_ptsd.asp#:~:text=PTSD%20Symptoms%20Can%20Be%20Affected,things%20most%20people%20consider%20safe.
[15] https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/how-does-coronavirus-affect-the-brain
[16] https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/how-does-coronavirus-affect-the-brain#:~:text=A%3A%20Cases%20around%20the%20world,Seizures
[17] https://www.frontiersin.org/research-topics/14627/impact-of-the-coronavirus-pandemic-covid-19-on-mood-disorders-and-suicide#:~:text=During%20the%20coronavirus%20COVID%2D19,problems%20and%20perceived%20social%20isolation.
[18] https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/how-does-coronavirus-affect-the-brain
[19] https://www.healthline.com/health-news/the-covid-19-symptoms-most-people-could-miss
[20] https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/how-does-coronavirus-affect-the-brain
[21] https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/how-does-coronavirus-affect-the-brain
[22] https://www.icudelirium.org/
[23] https://www.talktomira.com/post/what-are-the-long-term-side-effects-of-coronavirus-covid-19
[i] https://www.cdc.gov/coronavirus/2019-ncov/hcp/duration-isolation.html?deliveryName=USCDC_2067-DM35559
[ii] https://patientresearchcovid19.com/
[iii] https://docs.google.com/document/d/1KmLkOArlJem-PArnBMbSp-S_E3OozD47UzvRG4qM5Yk/edit
[2] https://www.technologyreview.com/2020/08/12/1006602/covid-19-long-haulers-are-organizing-online-to-study-themselves/
[3] https://docs.google.com/forms/d/e/1FAIpQLScM2EeJhgisTUdo5Op6euyx1PYu8O-aNeDVYhXuPFa_Gs9PnQ/viewform
[4] https://patientresearchcovid19.com/
[5] https://docs.google.com/document/d/1KmLkOArlJem-PArnBMbSp-S_E3OozD47UzvRG4qM5Yk/edit
[6] https://docs.google.com/document/d/1KmLkOArlJem-PArnBMbSp-S_E3OozD47UzvRG4qM5Yk/edit
[7] https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/how-does-coronavirus-affect-the-brain
[8] https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/how-does-coronavirus-affect-the-brain
[9] https://www.medpagetoday.com/neurology/dementia/87543
[10] https://health.ucdavis.edu/health-news/newsroom/covid-fatigue-is-hitting-hard-fighting-it-is-hard-too-says-uc-davis-health-psychologist/2020/07
[11] https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/how-does-coronavirus-affect-the-brain
[12] https://health.ucdavis.edu/health-news/newsroom/covid-fatigue-is-hitting-hard-fighting-it-is-hard-too-says-uc-davis-health-psychologist/2020/07
[13] https://www.ptsd.va.gov/covid/COVID_effects_ptsd.asp#:~:text=PTSD%20Symptoms%20Can%20Be%20Affected,things%20most%20people%20consider%20safe.
[14] https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/how-does-coronavirus-affect-the-brain
[15] https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/how-does-coronavirus-affect-the-brain#:~:text=A%3A%20Cases%20around%20the%20world,Seizures
[16] https://www.frontiersin.org/research-topics/14627/impact-of-the-coronavirus-pandemic-covid-19-on-mood-disorders-and-suicide#:~:text=During%20the%20coronavirus%20COVID%2D19,problems%20and%20perceived%20social%20isolation.
[17] https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/how-does-coronavirus-affect-the-brain
[18] https://www.healthline.com/health-news/the-covid-19-symptoms-most-people-could-miss
[19] https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/how-does-coronavirus-affect-the-brain
[20] https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/how-does-coronavirus-affect-the-brain
[21] https://www.icudelirium.org/
[22] https://www.talktomira.com/post/what-are-the-long-term-side-effects-of-coronavirus-covid-19
[i] https://www.cdc.gov/coronavirus/2019-ncov/hcp/duration-isolation.html?deliveryName=USCDC_2067-DM35559