Today, Is Your Client Prepared to Speak with Their Judge? What is the ‘1’ Thing that Differentiates Them from Everyone Else Entering Their Judge’s Courtroom?
Your Sentencing Hearing is a pivotal moment that could profoundly impact your future. You need to recognize that the Judge has already assessed your Presentence Report, which was created by your Probation Officer, and carefully considered your case. Additionally, the Judge has received a recommendation regarding your sentence. It’s imperative to understand that this hearing does not have to be a mere formality but an opportunity to present yourself in the best possible light and potentially influence your outcome. Take it seriously, and prepare accordingly. I hope this video is helpful and gives you a starting point to work with.
Facing America’s Criminal Justice System for the first time is a life-altering, surreal, and frightening experience. The importance of preparation and working with your legal team before the presentence interview cannot be overstated.
Once this has all been completed, as an attorney, you’ve prepped your client right up to their sentencing hearing.
Then, after sentencing, there still are a lot of fears and unknowns as they face either their self-surrender date or are remanded at that time.
Attorneys know the law, but the nuances of navigating through Federal Prison aren’t part of a traditional legal defense. This requires a unique set of knowledge and skills that interest those assessing a person’s access to freedom.
STAKEHOLDERSare part of the system that controls everything that happens following the guilty verdict and until you’re released from the Federal Bureau of Prisons. They are responsible for keeping society safe by reducing criminogenic needs for those who will eventually be released. From the Judge to the BOP Case Manager and Unit Team, to the Probation Officer on Supervised Release, and then possibly back again to the Judge to get off Supervised Release early, at each stage, these STAKEHOLDERS make decisions that impact your client’s future.
Realize that even if you’re doing everything right from the start, the only person you can control is – you, and still, there will be disappointments. Therefore, being prepared at every stage, keeping your eyes open with a positive attitude, and continuing to add to your Reentry Plan are all ingredients needed for getting home to your loved ones. Remember: No Cell Phones, No Trouble, and No Infractions.
In this video, I introduce you to your STAKEHOLDERS, who will be making decisions that determine and impact your immediate future. Some of these you will meet personally, while others, such as the BOP Staff located at the BOP Designation Center in Grand Prairie, TX, you will never meet. These two groups have in common that they will, for lack of a better term, profile you based either on (1) your INDICTMENT and Presentence Report or (2) Your Personal NARRATIVE, if it’s included with your Presentence Report and Indictment. Which do you suppose will portray you in the best light? I hope the video provides some clarity.
1. Your Judge, who already knows that;
Your Attorney is paid to keep you out of prison or, at best, spend the least time “in prison”.
The Probation Officer will conduct their interview, draft the Presentence Report, and recommend your sentence and placement to the court based on your interview. Currently, all they know about you is the Narrative provided by the DOJ through their Indictment of you – this, you can change.
The Prosecutor wants another conviction in his/her file. Currently, all they know about you is also the Narrative provided by the DOJ.
The DOJ wants Jail time.
But your Judge knows nothing about you – andonlyYour NARRATIVE can begin to change this, starting with1st)Helping the Judge Understand Who You Are– and why You Deserve Leniency – Selling your Luxury Cars, Homes, and other stuff if You Have Financial Penalties, 2nd)What Changed in Your Life – That Caused You to Break the Law?3rd)Invest In Yourself– You Can’t Change the Past, But You Can Change Your Future, start by writing your Story or Narrative.
2. Your Attorney, until now, also knows nothing about your background, but their time is mostly spent on your legal defense.
3. The Probation Officer will conduct your Presentence Interview and then write the official Presentence Report. But a week or so before your Presentence Interview, your attorney could provide your Probation Officer with your,
I. Copies of all of your Personal Identification and Biographical Background Information
Why be prepared with answers to the Assessment Questions? When you arrive at your 1st meeting with your Case Manager, these Assessments must be done and completed for your FSA Programs and Earned Time Credits (ETC) to be offered and then counted – without you taking the Assessment Survey, the programs cannot be offered.
During the interview, they can now ask questions and get to know you more personally.
Some may appreciate your efforts and become advocates since they are overworked and have no time.
4. TheProsecutor wants a conviction and only knows about you through the DOJ’s Narrative or your Indictment. Your Narrative may sway them, too.
5. The BOP Designation Center in Texas places you into a BOP Prison without ever meeting you.
6. Your Probation Officer during Supervised Release. To date, all they know about you is the Narrative released by the DOJ through their Indictment. Your Narrative and Release Plan can change that and your life.
CLIENT PREPARATION: THE WORK YOU DO – IS ADVOCATING FOR YOURSELF
The Personal Narrative, Reentry-Release Plan, and answers to the SPARC-13Assessment Questions(as you are expected to answer these questions when you first arrive, you might as well become familiar with them early), are written as one document and weaved into the Presentence Report when provided to your Probation Officer, a few weeks before your Presentence Interview.
Here, the defendant has accepted responsibility, expressed remorse for the victim(s) pain, suffering, and how it has impacted them and agrees with the court about the seriousness of the crime without minimizing it.
The caveat is that the defendant must put time and effort into writing their Narrative, Allocution, and Reentry Plan because their future depends on it being honest, pure, and from the heart.
PERSONAL NARRATIVE. Writing your story through Your Narrativetells the Judge how you came to this point in your life. This is an arduous, self-reflective experience for you to go through, forcing a face-to-face with your innermost thoughts. This is your autobiography (of you and those around you), the good, the bad, and the ugly. It may require you to enlist someone with federal sentencing mitigation experience to guide you in drafting your narrative, but this is the story of your client’s life and requires their participation. This short 3-4 minute video provides another way to think about when writing your Narrative.
NATURE and CIRCUMSTANCE You want to include: 1) What led you to do this, 2) How did you get involved, and 3) What was your involvement? [check that your involvement reflects what is in the official Presentence Report].
Taking weeks to months to complete can result in a distilled version of yourself that is honest and pure, where you feel Remorse, Accept Responsibility, and Identify with the Victims of the Crime You Perpetrated.
Mention if you have already started taking these before your Indictment or Presentence Interview (if applicable AA, NA, Gambling, or Sex offense) therapy and forensic (per your attorney, for example, Dementia, there is only ‘1’ Prison Nationwide with a very limited number of beds), therapy sessions.
If the resulting Narrative or Your Story – is quite the opposite of the DOJ’s Indictment Narrative, where you sounded like ‘America’s Most Wanted’, you did a Great Job!
REENTRY/RELEASE PLAN EXAMPLE.Include that you realize you need to learn from theFSA Risk Reduction Programsand implement their lessons into your daily life. Then expand on an appropriate theme, “Since my indictment, arrest, criminal charge, plea hearing, trial or guilty plea, presentence investigation, and sentencing process, I had the time to think about all that I have done. I made BAD decisions, except it shouldn’t be about ME – It’s about MY Victims and What I did. This is most important, as I must Prove my Remorse and my Efforts to Change and Accept Responsibility for The Pain I caused to my victims, the community, my family, and myself. To the court, I do not want to be here again – I have learned a hard and humbling lesson.
If you are currently taking FSA Programs for AA, NA, Gambling, or a Sex Therapy Program, where applicable when released, you want to continue the Therapy and Rehab for AA, NA, Gambling, or Sex therapy rehab. sessions. Write this.
You also have copies of your Social Security Card, Driver’s License (if expired, it needs to be updated with a new test likely), and Birth Certificate. You are grateful to be moving into a home with a support structure. While you have been self-employed forever, you have a letter from a friend willing to hire you, “all I have to do is let them know, as they are expecting my call from me.” “As you see, the letter was also a character letter that I initially provided.”
This YouTube covers Self-Advocacy or everything you can do before your Presentence Interview and then while incarcerated to help you expedite your way to freedom. While this sounds simple – It’s Not. You will be faced with many days of frustration and disappointment, and BOP staff who appear to be there just to give you a hard time. On the other hand, there will be those who care and will, over time, surprise you in good ways, yet unseen. While nothing can or is guaranteed, please use no cell phones, keep busy with constructive activities and non-fiction reading, and document everything that you you for your record. This video provides helpful content.
At the same time, you can also plan to be self-employed again if your role in that business was not part of your criminal charge. Then everything that goes into a traditional business plan, including what you would present to a bank, should be professionally (not handwritten, not expensive) put together, as your Probation Officer will want to see this during or before your Supervised Release.
ALLOCUTION. You maybegin by writing (in your own words) something like this…, “I am embarrassed and humbled to be standing here – since my indictment had the time to think about all that I have done, I didn’t recognize how BAD my decisions were, but Now I realized it’s Not About Me. It is about MY VICTIMS, What I did, and What I must do – to make it right. Please listen to this Short but direct YouTube.
Several memorable Statements/Allocutions that positively impacted these Judges,
“No punishment will be enough. If I could go back and change everything, I would.”
I am persuaded that the defendant is sincere and demonstrates insight into the crime.
Allocution is very important, “I’d like to have a conversation with the defendant.”
I want him/her to apologize to the victim and their family, mainly if they are in the courtroom.
“Allocution, however, changes this when I see the defendant has insight into the harm they have done,” when I see they have insight into this.”
“I am looking for remorse and insight as to why he did what he did and what he is doing to ensure that it doesn’t happen again.
As you stand at your sentencing hearing, nervous, anticipating the conversation with your Judge (your Allocution), you may also realize that writing your narrative has been an unexpectedly cathartic experience. Speaking from the heart could influence the court and ‘may’ impact your sentence…
CHARACTER REFERENCE LETTER. These are letters to one’s character; they know that you have broken the law and have known you for a long time. Should an employer be willing to write a letter that states they are still willing to rehire you after release from prison due to your ‘character and skills’ – that is a Great letter and should be included.
The ‘writer’ of a Character Letter states that they’ve known you for many years and are aware that you are in trouble and facing federal criminal charges and that you feel terrible about what you did. “We went to college together, and this is so out of character,” and they know that you are so remorseful. Further, as someone who is close to you and part of your support system, they want to assure this court that the defendant won’t be back in front of this judge again because we will be looking out for them in the future and hold them accountable. The video is short but goes into the do’s and don’ts of what goes into a Character Letter. Also, a great Character letter may be a letter that includes that a person will be willing to rehire you after your release due to your character, knowledge, and skills. In this video, I lay out the “dos and don’ts” of what to include in Character Reference Letters.
NOW,are you Better Prepared to Speak to The Judge at Their Hearing Regarding…What is the ‘1’ Thing that Differentiates Them from Everyone Else entering their Judge’s Courtroom?
You’re Now The Target of The FBI – What Are Your Options?
If you’re hearing FBI whispers,
Start interviewing attorneys, ask questions, get references, and ask to see several Sentencing Memorandums written for previous clients with similar legal challanges
Then, be honest with your attorney and yourself regarding your case. This is not a trick question, as it’s taken me time to see how I was at fault. Your attorney doesn’t want surprises because you are the only one who suffers.
PSI Preparationis crucial – You Are your best and only Advocate
Ask yourself long before your presentence interview:
• Do you have confidence in your defense?
• Do you need additional team partners who are specialized in, Sentencing Mitigation, Allocution, Personal Narrative and Reentry Release Planning and Advocacy
If Not,
· There are No Redo’s ⇒ this is Your Future ⇒ Speak up now
PREPARATIONand SELF-ADVOCACYare CORE VALUES
PREPARATION:
Attorney Interview, Working together – must be a Joint Project
Decision #1: Trial or Plea
PRACTICE Role Playing: Your Allocution and Your Attorney’s Statement for the Sentencing Hearing
Your Narrative isweaved into your conversation with your PO for placement into your Presentence Report (PSR), which is now complete.
SELF-ADVOCACY:
• Relies on the skills that made you successful, some being “Self-Motivated”
• At your Attorneys request, your Personal Narrative was included in Your PSR
• Reentry Planning
• Sentence Mitigation Strategies are employed before Sentencing and During Incarceration
YOUR PREPARATION
Working Together With Your Attorney At Every Stage
1st) Be honest with your attorney about everything – Plea or Trial – Nobody wants surprises
2nd) Your PSI needs to include everything about you.
In addition to all your Biographical Background information, Medical, Character References, Education, Legal, Etc.
Your attorney has connected with your PO before your Interview to get a “pulse” on how much they know, to present their case/defense strategy, and learn the date the PO must have their final PSR completed and submitted to their supervisor.
RDAP (if applicable): Include it now, because if it is not there, and you need it later to reduce your time, that may be a big lift.
Your Personal Narrative needs to be finished before your interview so;
That you know it, cold, and discuss it in 1st person with your P.O.
It should be able to be, copy-pasted directly into the P.O., Presentence Report
This Is Your Story: In Written and/or Video Format
3rd) Time must be allowed for the development of your Personal Narrative.
4th) The PSR is Now Complete and should Include all the Above, including your Personal Narrative – which Judges want to see.
5th) Time is spent practicing your Allocution for your sentencing hearing with your attorney.
1. If the Judge is aggregable, due to your allocution, they may Depart below the guidelines
2. If RDAP is applicable (it’s referenced in your Presentence Report) now, your attorney can ask for it to be put into the order, and if the judge agrees, then
3. Politely, also request for 1 specific BOP prison, based on a specific BOP program (camp eligible < 10 years), also to be put into the order.
Additionally, if the BOP is unable to make the placement, could they inform the court why, in writing?
SELF-ADVOCACY Allocution – Your Personal Narrative
Judge Jon D. Levy of the District of Maine in Portland,
Judge Patti Sarrisof the District of Massachusetts
Judge Cynthia A. Bashant;
Judge Morrison C. England Jr;…one of the biggest mistakes defense lawyers can make is not having their client answer the question…
Judge Lawrence C. O’Neill,
Judge James K. Bredar—says he comes out on the bench with a sentence already in mind. “Allocution, however, changes this when I see the defendant has insight into the harm he has done.”
NACDL, The Champion • March 2011, Heartstrings or Heartburn: A Federal Judge’s Musings On Defendants’ Right and Rite of Allocution,
Judge Mark Bennett: A Good Allocution Can Be Beneficial
Here’s what Federal Judges Want To Hear
We’re interested in a defendant who has the capability of introspection and who has come to grips with the impact of his offense on others
“No punishment will be enough. If I could go back and change everything, I would.”
I am persuaded that the defendant is sincere and demonstrates insight into the crime.
Allocution is very important, “I like to have a conversation with the defendant,”…
I want him to apologize to the victim and his or her family, particularly if they are in the courtroom.
“Allocution, however, changes this when I see the defendant has insight into the harm he has done,” when I see the defendant has insight into the harm he has done”
“I am looking for remorse and insight as to why he did what he did and what he is doing to make sure that it doesn’t happen again.
“It’s very important that lawyers prepare a client for allocution, even if they have gone to trial and do the job that they are retained to do.”
Start paying restitution, even $25/mo, and don’t show up at court in a $900 luxury car.
You’re Now The Target of The FBI
You Have A Choice
PREPARATION FOR A SUCCESSFUL LIFE AFTER RELEASE
Marc
240.888.7778 Physician Presentence Report Service
No matter where you are in The Process, there are things we can do.
* No Physician, Attorney, or Consultant can promise any outcomes.
But what that means and how to get needed treatment is often not well understood by attorneys representing criminal defendants.
This article attempts to address that knowledge deficit by explaining the;
Medical, mental health, and substance abuse programs and,
Policies in the federal Bureau of Prisons (BOP), as well as some of the,
Educational, vocational, and other available programs intended to rehabilitate inmates and prepare them for return to society.
Equally important, the article explains;
The critical role of the presentence report (PSR) in determining,
Whether and how needed treatment and programs will be available to a defendant.
Documentation is paramount, and,
The diligent attorney must be proactive in gathering and supplying the appropriate documentation to,
The probation officer preparing the PSR and to the court, along with,
A sentencing memorandum advocating for the defendant’s desired,
Sentencing outcome and institutional placement,
Supported by the sentencing factors set forth in 18 U.S.C. § 3553(a).
The PSR plays a critical role in a defendant’s post-conviction life.
In federal court,
The sentencing judge relies on the report to determine sentencing guidelines, departures, and statutory sentencing considerations under 18 U.S.C. § 3553(a).
The BOP
Relies on the PSR to make decisions about custodial placement, security classification, educational/vocational needs, and medical/psychological treatment needs.
On supervised release after incarceration,
The PSR influences the probation officer’s supervision of the defendant and the requirements of supervision. In short,
The PSR is now part of the defendant’s permanent record and is considered the gospel truth about the defendant. It truly is
“The gift that keeps on giving,” so accuracy is key.
Given the PSR’s permanence and omnipresence,
One cannot overstate its importance or the need for accuracy. Counsel must
Object to inaccurate facts and omissions of important information in the report.
Once the court has made final rulings on all objections, and
Before the PSR is sent to the BOP, counsel must ensure that the report is updated in accordance with the court’s ruling.
Asking to amend the PSR later, when an inmate is already in the BOP,
Asks a court to change positions that it has already adopted as accurate.
Even if this can be done—a big if—the amendment process can take years and many attorney hours to complete.2
Components of the Federal PSR
First and foremost,
The PSR provides details about the offense for which a defendant is being sentenced,
Whether the defendant has accepted responsibility for his or her conduct, and
How the sentencing guidelines apply.
The report also contains some
Background information about the defendant that the court may consider in deciding what sentence to impose, including
Prior criminal history,
Educational background,
Work history,
Family background, and health.
Many attorneys seem to forget, however, that sentencing is only one purpose of the PSR.
The BOP initially relies on the PSR to determine, a defendant’s security classification and whether to house the inmate in a high-security U.S. penitentiary (USP), a medium or low-security federal correctional institution (FCI), or a minimum-security prison camp.
The BOP also determines whether a defendant has
Medical or mental health needs that affect placement.
Continuity of care in the BOP, to the extent it will happen, depends on an accurate PSR.
The PSR acts as a
“Medical referral” for the client based on his or her
Medical and mental healthcare history,
Current medications, and
Security referral regarding their requirements.
The PSR needs to be as complete as possible to reduce unnecessary lapses in medical care.
Finally, the PSR can provide information about a defendant’s
Educational, vocational, and avocational interests, can
Facilitate placement in a facility with appropriate programs to enhance rehabilitation and successful return to society.
By knowing what programs and treatment the BOP provides, an attorney can better assist the client in making sure the PSR has appropriate documentation to improve the chances of a client’s placement in the most appropriate location.
A defendant has a constitutional right to adequate health care.
This means that prisons must provide necessary medical attention and may,
Not act with deliberate indifference to a prisoner’s pain and suffering.3
The BOP attempts to meet its constitutional obligation efficiently and cost-effectively by having inmates placed at different facilities based on their
Medical CARE LEVEL.
All BOP facilities have staff members who are trained as first responders to use the automatic external defibrillator and to perform cardiopulmonary resuscitation in emergency situations.4
As an inmate first enters the BOP system, the Designation and Sentence Computation Center enters the defendant’s information, including
criminal history, offense, sentence, medical documents, and treatment history from the PSR
into their SENTRY software to
determine both
security classification and
medical care level designation for that inmate.
Designations range from
CARE LEVEL I for the healthiest inmates to
CARE LEVEL IV for gravely ailing inmate-patients needing inpatient care.
An institution designation is then determined, based on the appropriate medical care level and security classification level. Final placement decisions for those inmates with significant health concerns/conditions are made by the Office of Medical Designation and Transportation at the BOP.
Medical CARE LEVELS in the BOP
Care Level I
Is comparable to the care provided by a general practice physician
Here one rarely visits for the occasional minor illness or injury.
For inmates who are less than 70 years old and healthy, with limited medical needs.
Stable mental and physical health and
Typically need physicians no more than once every six months.
Mental health crises would be of short duration and
would not require hospitalization.
Examples of “limited” medical needs include;
Mild asthma,
Diet-controlled diabetes, and
Stable HIV for which medications are unnecessary.
A community hospital is usually approximately one hour away.
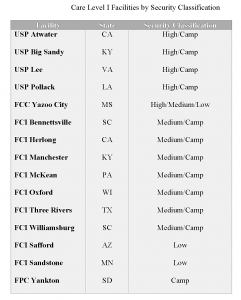
See Table 1 for BOP Care Level I facilities, grouped by security classification.
Most federal prison facilities are designated Care Level II
This is the level of care needed by the majority of people.
These facilities provide medical care similar to a fully staffed internal medicine practice.
Some chronic illnesses or those requiring regular medication, but their
Health is generally stable, and hospitalizations are not usually required.
Inmates may have a mental health diagnosis requiring
routine outpatient care,
controlled with medication or talk therapy.
Medical or psychological patient care visits may be available monthly to quarterly.
The Care Level II facilities are within one hour of a regional hospital center, but
the need for hospitalization for such an inmate would not be expected more than once every two years. See Table 2 for BOP Care Level II facilities, grouped by security classification.
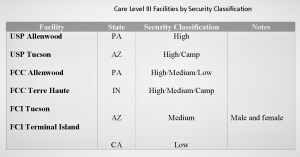
Care Level III facilities are located near a major community medical facility to ensure outside necessary medical care is within close proximity to the designated institution. Care Level III inmates include those needing “companions” to help with their activities of daily living (but not needing daily nursing supervision) and those needing daily to monthly medical or psychiatric visits.
Other Care Level III inmates include those suffering from cancer in remission of less than one year, advanced HIV, severe mental illness in remission on medication, congestive heart failure, and end-stage liver disease. These inmates may have chronic or recurrent mental illnesses or ongoing cognitive impairments. Daily inpatient nursing care is not available, but inmates at this care level may require hospitalization periodically to stabilize their medical or mental health conditions enough to keep them from deteriorating to the point of requiring around-the-clock nursing care. See Table 3 for BOP Care Level III facilities, grouped by security classification.
Care Level IV facilities are known as Medical Centers For Federal Prisoners (MCFP) or Federal Medical Centers (FMC). They operate like small hospitals and provide varying degrees of nursing and medical care, including surgical, diagnostic, and therapeutic services. They are the only BOP facilities able to provide Care Level IV inmates with the around-the-clock nursing care needed for acute
medical or chronic mental health conditions resulting in severe physical and cognitive impairments. Physical ailments designated to this level include end-stage kidney failure (requiring dialysis), unremitted cancer, quadriplegia, stroke, debilitating neurological trauma, major surgery, or high-risk pregnancy, and recent transplant recipients (within one year). Mental health diagnoses so severe that an inmate cannot function in the general population may be designated to a mental health unit within one of the prison medical facilities. Care Level IV facilities accommodate inmates of every security level, which makes the safety of a nonviolent offender an issue to be raised. See Table 4 for more detailed information about the BOP Care Level IV facilities.
Scope of Services Covered
Federal prison healthcare is implemented through a mix of BOP employees and public health service officers. Primary responsibilities fall on the primary care provider team, which provides medical care to inmate patients under a medical or clinical director’s supervision.5 This is the BOP’s equivalent of a staffed medical practice.
Working under staff physicians (and psychiatrists at selected facilities), mid-level practitioners include registered nurses, licensed practical nurses, licensed vocational nurses, nurse practitioners, physician assistants, and certified nursing assistants. These staffers are in turn supported by general laboratory technicians, like X-ray technicians and phlebotomists, as well as not-yet-licensed foreign medical school graduates. EMTs also act as mid-level practitioners. Additionally, all facilities have a dentist and may have contracts with orthopedics, neurologists, optometrists, and other specialists from the local community who come to the prison for onsite medical visits. Mid-level practitioners are the inmate-patient’s primary point of contact. They serve as the primary care provider for routine requests, new complaint evaluations, and ongoing management of recur- ring conditions, and emergencies.
The BOP sorts medical treatment into five categories, which can objectively be called:
1. Life-Threatening Conditions
Treatment for life-threatening conditions is essential to sustain the life or function of a critical bodily system and requires immediate attention. The BOP refers to these conditions as “Medically Necessary–Acute or Emergent” and includes the following conditions in this category: heart attacks, severe trauma such as head injury, hemorrhage, stroke, detached retina, sudden vision loss, and complications of pregnancy or labor.7
2. Medically Necessary Conditions
The BOP defines this category to include conditions that are not immediately life-threatening but which without treatment now, the inmate could not be maintained without significant risk of:
Serious deterioration leading to premature
Significant reduction in the possibility of repair later without present
Significant pain or discomfort that impairs the inmate’s participation in activities of daily 8 Examples of conditions the BOP includes here are chronic conditions such as high blood pressure, high cholesterol, heart disease, and diabetes; severe mental health issues (e.g., bipolar disorder, schizophrenia); infectious disorders (e.g., HIV, tuberculosis); and cancer.9
3. Medically Necessary but Not Urgent
The BOP actually defines this category as “Medically Acceptable— Not Always Necessary.”10 The group includes conditions for which “treatment may improve the inmate’s quality of life.”11 Examples of treatments for conditions in this category, as listed in the BOP Policy on Patient Care, include joint replacements, reconstruction of the anterior cruciate ligament (ACL) in the knee, and treatment of noncancerous skin conditions.12 Such treatment procedures require review and approval by the institution’s Utilization Review Committee, which considers various factors, including risks and benefits of the treatment, available resources (including the cost of security staffing and transportation), the inmate-patient’s medical history, and how an intervention (or lack thereof ) will impact the inmate’s activities of daily living.13
Should an outside specialist consult be needed for a nonemergent condition, a referral request is made to the prison’s Utilization Review Committee and clinical director. Other members involved in this decision-making process include the associate warden or warden, health service administrator or assistant, the medical trip coordinator, any health care providers directly involved in the referral, and perhaps the director of nursing and the chaplain or a social worker.14
The clinical director has the final say over all Utilization Review Committee decisions.15 If approved, the inmate-patient will be placed on a schedule or waitlisted until the specialist has an opening during the contract’s limited monthly hours, which may be several months or years later. Notably, the clinical director is under no obligation to follow medical recommendations made by the outside physician consultant specialist. If the recommendations are not followed, the clinical director will document his/her justification in the inmate’s health record.16 Justification may be based on the category of care sought.
4. Medically Appropriate
Some treatments, even though recommended by a health care provider and deemed appropriate by the clinical director, still require approval by the Utilization Review Committee, which is not likely to be granted. These treatments are considered by the BOP to have “limited medical value” and include cosmetic procedures and the removal of noncancerous skin lesions.17 It is worth noting that some skin lesions may be misdiagnosed, so the denial of treatment for these appropriate medical procedures is a concern for inmates with such health needs.
5. Extraordinary Treatments
The BOP considers a medical treatment extraordinary if it “affect[s] the life of another individual, such as organ transplantation.”18 Thus, organ transplants and experimental/investigational treatments require approval of the Utilization Review Committee, which is not likely to be granted.
Medical Devices and Pharmaceuticals
If an incarcerated inmate needs medical devices, glasses, prosthetics, or other medical support items, these can be mailed directly from his or her personal physician’s office or a medical business (e.g., Pearl Vision) with the attached physician orders and using form BP-AO331.19 These items cannot be mailed by family members, friends, or other nonmedical civilians. Prescription eyeglasses, medical devices (such as CPAP or BiPAP, or other machines for sleep apnea), prosthetics, and similar devices should also be brought with the patient, along with doctors’ prescriptions and orders. The PSR should also mention that the defendant has these devices pursuant to medical orders. If the client does not take these devices with him or her when reporting, he or she may have to wait several weeks for the BOP to obtain appropriate medical devices; the inmate’s family will not be allowed to mail/send the items to the facility, as they must come directly from a medical company or health care provider.
If the inmate regularly takes prescribed medication, the BOP will usually substitute generic medications for brand-name drugs. Not only does BOP policy generally require generic medications, but BOP medical personnel, pharmacists, and consulting physicians are required to use “the least expensive generic equivalent … when available.”20 Thus, instead of generic equivalents, the BOP may prescribe an alternative (but less expensive) generic medication that is for the treatment of the same medical condition. Much like insurance companies, the BOP has a formulary of approved medications.21
The formulary includes the generic name of the medication, what conditions it may be prescribed for, acceptable dose levels, and limits on the number of days the medication can be prescribed.22 Use of any medication that is not on the formulary or use of a medication in a different manner, for treatment of a different condition than authorized by the formulary, or longer than authorized, requires pre-approval from the BOP medical director, after going through the institution’s clinical director and the BOP regional medical director—an extensive and lengthy process.23 Some nonformulary drugs are available only in limited circumstances, such as the preferred medication’s failure to work for the patient, but only after the lengthy pre-approval process. Some medications, such as opiate narcotics, are only available in Care Level IV facilities for very limited circumstances; those medications and psychiatric medications must be crushed by the health care provider and administered to the patient in the provider’s presence.24 This is to prevent diversion of the medication by inmates for unlawful purposes. Prescribing medication without pre-approval is considered an unauthorized use of government funds, a felony offense.25
In short, the medications the patient-inmate receives in custody will not necessarily match the medications that the inmate received before incarceration. Even if the inmate is lucky enough to be taking the same medications as before, a variety of manufacturers will pro- vide the same generic drug in different colors, sizes, and shapes than the inmate may have been used to. To avoid unnecessary anxiety and surprise for the client, an attorney should educate his or her client about these BOP policies. If a client is on nonformulary medication, the attorney needs to assist the client in obtaining pre-approval before arrival at the facility, which takes substantial time, in order to prevent unnecessary and potentially harmful interruption of the client’s medical treatment.
If a client is self-surrendering to the BOP, he or she should bring along a three to four-week supply of his or her medication in original, properly labeled bottles. These prescriptions may ultimately be returned to the client’s home, but at least they will be available if needed for continuity of care purposes, in case the institution does not have the correct medication in stock.
Programming in the Federal BOP
In the last century, American society transitioned from institutionalizing people with mental health conditions in mental health facilities (often underfunded and operating under poor conditions) to incarcerating the mentally ill in jails and prisons.26 Nearly 50 percent of jail inmates and over one-third of prison inmates suffer from mental health problems.27 Mental illness often underlies behavioral problems, and if an incarcerated inmate has not been properly diagnosed or given treatment for a mental illness, chances are high that the inmate will be involved in fights, assaults, self-injurious behavior, or other misconduct in prison that leads to disciplinary consequences, including restrictive housing units;28 use of restrictive housing units, especially solitary confinement, exacerbates mental illness rather than helping the inmate.29
Therefore, it is imperative that the defense attorney makes sure that psychiatric and psychological issues are identified and included in the defendant’s presentence report, along with the appropriate treatment plan recommended by a qualified psychiatric health provider. If mental health issues are apparent, but the defendant has no documentation of diagnosis or treatment, the attorney should obtain a professional psychological evaluation before the probation officer begins preparing the PSR. Failure to do so will consign the defendant to an increased risk of restrictive housing or solitary confinement. When requesting placement in a specific facility or program, the defense counsel should ask the court not only to recommend the placement but to include the reasons for his recommendation, which will improve the chances of securing the placement. One additional measure to possibly increase the chance of the BOP following the recommendation of the court is to ask the sentencing judge to order the BOP to provide in writing, the reason for not following the judicial recommendation.
Documentation of known mental health issues and treatment (including substance abuse and addiction) is essential for continuity of care. Without documentation of the diagnosis and need for specific medication in the PSR, for example, an inmate entering the BOP will have no access to medication.
In that case, there will be a waiting period, sometimes several weeks, before the inmate will be seen and evaluated, and prescribed a medication deemed suitable by the prison medical establishment. During the delay without any medication, the inmate’s condition is likely to deteriorate. In addition, when providing the substance abuse history, it is imperative that the PSR document frequency and current substance use activity. Upon initial remand or voluntary surrender to the assigned prison, the defendant may require placement in an institution that is equipped to provide a safe detox environment. If the BOP is unaware—from documented medical records in the PSR—that some medications have been unsuccessful, the patient-inmate may be doomed to another trial period of medication already known to be ineffective for him.
Beyond access to basic mental health care and medication, documentation of known mental health and related conditions is necessary for inmates to be eligible to participate in some programs. The BOP offers a variety of programs to provide mental health support, substance abuse education and treatment, continuing education, and vocational training. Other programs help inmates adjust to prison life, develop coping skills, or heal from past trauma that may have played a contributing role in an inmate’s criminal conduct. However, some of the programs have the minimal capacity and are offered only at certain facilities. If a defendant’s need and desire for a particular program are made clear in the PSR, his or her chances for placement at a facility offering the program will be improved. Addressing program needs with the assigned assistant U.S. attorney before sentencing and obtaining the government’s agreement to recommend the placement will also improve the defendant’s chances. These programs are discussed in this section.
Programs Promoting Psychological Well-Being
1. The Mental Health Treatment Programs
The BOP has a series of residential Mental Health Treatment Programs to treat inmates diagnosed with serious mental illness and behavioral disorders, particularly for inmates who do not require hospitalization but nonetheless need intensive treatment services and/ or lack the ability to function in a general population setting. These programs include the Habilitation Program, the Skills Program, the Axis II Program, and Mental Health Step-Down units.30
TheHabilitation Program is for high-security inmates who lack the ability to adapt to the penitentiary environment because of mental illness, but who may be able to function in a medium-security environment with proper residential treatment.31
The Skills Program is for inmates with both mental illness and cognitive/intellectual limitations that limit their ability to adapt to living in the community and in prison.32 The program is currently available at FCI Danbury (Low) and FCI Coleman (Medium). The Skills Program has evolved into a residential program that now has an emphasis on addressing the needs of offenders who are determined to be on the Autism Spectrum. This 12-18 month program assists in providing inmates on the autism spectrum with coping mechanisms and tools to be able to manage better once released from the program and assigned to the general population.
TheAxis II Program is for inmates with Borderline Personality Disorder or other severe personality disorders who have a history of behavioral problems in the prison, but who are amenable to treatment.33 More recently, this program, also known asSTAGES (Steps Toward Awareness, Growth, and Emotional Strength). The program is designed to increase the time between disruptive behaviors, foster living within the general population or community setting, and increase pro-social skills. The Stages Program is available at FMC Rochester, USP Florence, and FCI Terre Haute.34
Mental Health Step-Down Units provide intensive treatment for inmates recently released from in-patient psychiatric hospitalization. Sometimes, inmates are placed in these units in an effort to avoid the need for in-patient hospitalization.35
Acceptance into any of the Mental Health Treatment Programs requires a diagnosis of mental illness or behavior disorder and a demonstrated need for intensive treatment (demonstrated by prior psychiatric hospitalizations/interventions, complex treatment with psychotropic medication, major functional impairment, or repeated incidents of severe behavioral problems in prison). Inmates in a residential treatment program reside together in a unit, with their living areas being separate from the general population, allowing the inmates to create a therapeutic community environment.
Most of their other activities, recreation, work assignment, and meals are shared with the general population inmates assigned to that particular facility. This placement also helps to protect mentally ill inmates from injuring themselves, from being victimized, and from being negatively influenced by peers in the general population. Inmates in these residential programs are still subject to being victimized; however, the potential for victimization is reduced. Unfortunately, the BOP has very limited capacity and lengthy waiting lists for placing inmates in one of these programs. With such limited capacity, the need for thorough documentation of prior mental health history in the PSR is readily imperative. Without the documented need for special placement, an inmate will be placed in the general population, with greatly increased chances of restrictive housing, isolation, and other counter-productive sanctions rather than treatment.
2. The Resolve Program
The Resolve Program is a cognitive-behavioral program designed to address the trauma-related mental health needs of inmates. Specifically, the program works with those who have previously been victims of child abuse or neglect, sexual assault, domestic violence, or other trauma is known to correlate with psychological disorders. Starting with an eight-hour workshop, the program is followed by six months of nonresidential treatment and seeks to decrease the incidence of trauma-related pathology and improve inmates’ level of functioning.36 Since 2007, the Resolve Program has been implemented at all BOP facilities housing women (except during times when the institution lacks a psychologist to lead the program).37 The program is available for men at the maximum security prison in Florence, Colo., and at FCI Danbury (Low) in Connecticut.38
3. The Challenge Program
The Challenge Program is a residential cognitive-behavioral treatment program developed for male inmates in penitentiary settings. The Challenge Program, which lasts at least nine months, provides three phases of treatment to high-security inmates with substance abuse problems and/or mental illness. Like the Mental Health Treatment Programs, participants live together in a unit separate from the general population. Incentives and rewards are available for the successful completion of all phases of the program.39 The program is available at several BOP facilities, but not at all of them.
Substance Abuse Programs
The BOP offers several different options for those inmates dealing with substance abuse issues, ranging from education to intensive treatment.40
1. Drug Abuse Education
Drug abuse education includes a series of classes providing education about substance abuse and its unwanted side effects. The classes may help identify offenders who need more than education.41 Any inmate is eligible to participate in drug abuse education classes, as long as he or she is not already enrolled in or has not already completed the residential drug abuse treatment program and has enough time remaining in custody to complete the course. The course is available at all BOP institutions.
2. Nonresidential Drug Abuse Treatment
Nonresidential drug abuse treatment is a 12-week cognitive-behavioral therapy, treatment program, usually conducted in group-therapy sessions. The program addresses the link between substance abuse and criminal lifestyles and provides opportunities for building and improving skills in rational thinking, communication, and community adjustment. The program is intended for inmates with relatively short sentences, those transitioning to the community, those who have failed a urinalysis drug screen, and for addicts in need of substantial treatment who are on the waiting list for the RDAP intensive treatment program or who are not eligible for RDAP.42 All BOP institutions have this program, which is open to any inmate who volunteers.43
3. Residential Drug Abuse Program (RDAP)
RDAP is an intensive residential treatment program, followed by transitional treatment in the community following release. Inmates in the program live in a prison housing unit separate from the general population in a modified therapeutic community setting. They spend half of each weekday in treatment, including individual and group counseling, and the other half of each day is spent in school, work, or vocational training.44 This portion of RDAP must last at least six months.45 The usual length of time of the residential portion of the treatment is approximately 10 months.
To be eligible for RDAP, the inmate must have a verifiable substance use disorder that was active within one year of the offense for which he or she is incarcerated.46 This means for eligibility, the offender must have been actively using substances within one year from the date of the arrest. For this reason, it is critical for the PSR to document active substance abuse and any prior efforts at treatment. Details of where and when treatment in the community was obtained should also be documented in the PSR for easy reference. A defendant who denies having a substance abuse problem during his or her presentence interview will have a much harder time establishing eligibility for the program later. An inmate must also sign an agreement to comply with program responsibilities and requirements; finally, an inmate must have sufficient remaining time on his or her sentence to complete the full program, or admission to the program will be denied.47
The RDAP program is widely sought because studies have demonstrated its effectiveness in preventing relapse to drug use and in reducing criminal recidivism.48 The program is also popular because eligible inmates who successfully complete the program can reduce the length of their prison sentences by 10 percent, up to a maximum of one year.49 Because of the program’s popularity, there is a waiting list to get into RDAP, and not all who need the program can get it.
There are also eligibility requirements for early release, such that not every participant in the program will receive the benefit of early release under 18 U.S.C. § 3621 (e). Those ineligible for early release include illegal aliens; pretrial detainees; military inmates or state inmates serving time in a BOP facility; inmates who previously completed the program and got an early release the first time; inmates currently serving a sentence for any violent felony, sex offense involving a minor, or any attempt, solicitation, or conspiracy to commit such violent felony or sex offense; and inmates with a detainer and inmates with a previous conviction (within 10 years of the sentence on current offense) for homicide, rape, robbery, aggravated assault, arson, kidnapping, or sexual abuse of a minor.50
Sex Offender Programs
The BOP offers sex offender treatment programs for inmates serving criminal sentences and for those who have been civilly committed as predatory sex offenders suffering from mental illness that renders them dangerous to the community.
1. Nonresidential Sex Offender Treatment Program
The non-residential sex offender treatment program consists of outpatient groups meeting two to three times per week for a total of six to eight hours per week. Completion of this moderate-intensity program takes at least nine months. Participants learn basic skills and concepts to help them understand their past offenses and to reduce the risk of future offenses. Eligibility for this program is limited to offenders who have been evaluated and found to have a low to moderate risk of re-offending. Attorneys should advise clients that the BOP uses this program to identify persons likely to re-offend; therefore, participation carries risks. However, failure to participate, if recommended by the BOP, can result in a loss of good-time credit. The non-residential sex offender treatment program is available at FCI Elkton, FCI Englewood, FCI Marianna, FCI Petersburg, FCI Seagoville, USP Marion, and USP Tucson for male offenders and at FMC Carswell for female offenders.51
2. Residential Sex Offender Treatment Program
The residential sex offender treatment program involves high-intensity programming for a period of 12 to 18 months. The BOP provides this program at FMC Devens in Massachusetts. Participants benefit from a therapeutic community in a residential housing unit where they work to reduce their risk of future offending. Offenders receive treatment five days per week. The program is targeted at offenders with an elevated risk of re-offending.52
Inmates who have served their sentences but are deemed at high risk of re-offending because of severe mental illness can be involuntarily committed to the custody of the attorney general for continued confinement and treatment.53 Some defense attorneys may advise their clients not to participate in sex offender treatment programs because information disclosed in treatment has sometimes been the basis for seeking an order of civil commitment.54
Policies and Programs for Pregnant Inmates
Female inmates are medically screened for pregnancy upon admission to the BOP, and they are instructed to inform medical staff immediately if they suspect they are pregnant.55 The BOP provides female inmates with medical and social services related to pregnancy, birth control, and child placement, as well as access to abortion. If necessary, childbirth takes place at a hospital outside the institution.56 Previously, an inmate could be handcuffed during delivery, but a provision of the First Step Act now prohibits such use of restraints except in limited circumstances.57 Outside social service agencies are contacted to help the inmate find an appropriate placement for the baby. Newborns are not allowed to return to the prison with their mothers, but they can accompany an adult visitor to the prison for visitation, in accordance with the prison’s visitation policies.
Attorneys representing a client who is pregnant or has a young child need to be aware of two special situations in the BOP discussed below.
Abortion
Federal law popularly known as the “Hyde Amendment” prohibits the use of federal funds to perform or facilitate abortions except where the mother’s life is endangered or in cases of rape or incest.58 This law applies to and is followed by the BOP.59 Pursuant to 28 C.F.R. §551.23, a pregnant inmate receives medical, religious, and social counseling about her pregnancy decision. If she decides to have an abortion, arrangements are made for these medical services to be provided at an appropriate clinic outside the institution, at the inmate’s expense (or her family’s). Even though not paying for the abortion procedure, the BOP may pay to escort the inmate to the procedure. Under BOP policy, BOP employees may decline to participate in the provision of abortion counseling or services, including transportation.60
The MINT Program
MINT (Mothers and Infants Nurturing Together) is an alternative residential program for low-risk female inmates who are pregnant when they arrive in prison. Eligible female inmates can enter the program two months before their delivery due date, and they can remain in the program for three months after the baby is born.61 The program’s purpose is to promote parent-child bonding and to improve parenting skills for the new mother. The program is administered through the Community Corrections Centers (CCC) and Residential Re-entry Centers (RRC), and the inmate must qualify to participate. A woman with more than five years to serve, who gets pregnant while incarcerated, or who plans to place the child for adoption is not eligible for the program, nor are sex offenders; deportable non-citizens, those with pending charges or a history of violence, or those requiring psychiatric hospitalization.62 Another requirement is that the mother is able to provide financial support for herself and her child (so that the BOP does not have to pay), but she may seek help from Social Services.63 Prior to the child’s birth, the mother must make custodial arrangements for the child, because, after the three-month bonding period, she must return to her original prison to finish her sentence.64 The CCC or RRC provides psychological counseling, drug counseling, and parenting classes.
One facility differs from the other federal MINT programs: Greenbrier Birthing Center, overseen by the Baltimore Residential Reentry Office, operates under a contract with the BOP. A female may remain at Greenbrier for up to 12 months with her child after birth. Located in Hillsboro, W. Va., the program seeks to provide a “home-like environment” to promote bonding and parenting skills. The facility has 20 private bedrooms, with every two rooms sharing a bathroom. The common area has a kitchen, recreation room, education room, physical training area, laundry facilities, and a phone room. Greenbrier also offers more programming than the minimum required by the BOP; in addition to parenting classes, psychological counseling, substance abuse counseling, and weekly screening, Greenbrier provides life skills classes, financial management, job readiness, and GED classes and testing onsite, all of which are intended to motivate and help the mother provide a stable environment for the child upon her release from custody.65
BRAVE Program
The BRAVE Program (Bureau Rehabilitation and Values Enhancement) is for young male offenders serving their first federal sentence. To qualify for the program, an inmate must be 32 years of age or younger, with a sentence of five years or longer, and federally incarcerated for the first time. The program utilizes a cognitive-behavioral approach to promote favorable institutional adjustment, positive interaction with staff members, and self-improvement activities. During the six-month residential program, inmates live together in a unit, completing an Orientation Phase, Core Treatment Phase, and Transition Phase.66 The BRAVE Program is offered at FCI Beckley and FCI Victorville-medium.
Educational Programs
An adult literacy program leading to the completion of a GED is available in each BOP institution. Inmates without a verified high school diploma or GED certificate who have the capacity to obtain one are expected to work towards completion of this program while incarcerated.67 The Warden at each facility is also to ensure the availability of an English as a Second Language program for non-En- English-speaking inmates who score below eighth-grade proficiency in reading and listening comprehension in English.68
The BOP Program Statement on Education notes the goal of providing postsecondary educational opportunities and adult continuing education classes for inmates.69 Individual classes in typing, computer literacy, and parenting skills are available as continuing education courses, but the reality is that … [2nd Chance Act for Incarcerated Individuals allowed eligible students in college-in-prison programs to access Federal Pell Grants beginning on July 1, 2023] Some BOP facilities have access to community college programs in which professors come to the facility to teach classes, and some have correspondence school options available to inmates. The attorney for a defendant who hopes to obtain some collegiate education should check the handbook for facilities where the client is likely to be placed to determine what advanced programs, if any, are available at the institutions.
Vocational Programs
The BOP endeavors to provide vocational education opportunities for inmates with limited employment history and few marketable skills. Vocational training is available in the form of apprenticeship programs, certificate programs, and on-the-job training in various fields.70 Popular apprenticeship programs include HVAC, electrical, and welding. The same programs are not available at every facility, however, and an attorney should determine which facilities offer a program that the client wishes to learn.
Conclusion
A defendant’s legal team must determine what medical and nonmedical information needs to be included (or not included) in the client’s presentence report. The goal is to request the client’s placement in a facility appropriate to his or her security classification, taking into consideration the defendant’s medical, psychological, and educational/programming needs. Accuracy and documentation of information from the beginning of representation is key to accomplishing this goal. Further, it is advisable for the legal team to call the classification center in Grand Prairie or to speak with staff at specific facilities to verify that desired programs are still available at that facility. Individual facilities sometimes “supplement” BOP practices based on local needs and resources, without public notification. Particularly if the defendant may be placed in a private contract facility, the attorney needs to learn about the programs, medical resources, and mental health care available at that facility and the requirements for eligibility. Most low-security non-U.S. citizen inmates are placed in one of the BOP’s contract for-profit prisons. Only by knowing the client’s needs and obtaining the appropriate documentation for the presentence report can the attorney give a defendant the best shot at receiving appropriate treatment and programming while incarcerated. 8
Dr.MarcBlatstein(info@pprsus.com)hada successful podiatric medical practice for 30 years providing quality patient care. In 2006, he was convicted of felony mail fraud and served one year and one day in prison for the actions of his office billing department’s use of incorrect billing codes. He maintains an active medical license and is the founder of Physician Presentence Report Service, LLC.
Fay F. Spence is an attorney with more than 30 years of experience in criminal law. She currently serves as a pro se law clerk for the U.S. District Court for the Western District of Virginia.
E.J. “Jay” Hurst II (jayhurst@jayhurst.net) has worked with BOP inmates and federal defendants since2001.Besidescriminaldefenseandpost-convictionlaw,Hurstpursuesfederal governmentrecordsundertheFreedomof Information Act and will periodically go to court on civil rights matters.
Maureen Baird (moiep@aol.com) served as warden at the Federal Correctional Institution in Danbury, Conn., and at the Metropolitan Correctional Center in New York City. While there, she was appointed to senior executive staff by the U.S. Attorney General. She then became warden of the U.S. Penitentiary in Marion, Ill.
4Fed. Bureau of Prisons, Patient Care 9 ( June 13, 2014), www. bop.gov/policy/progstat/6031_004.pdf.
5Id. at 13-14.
6Id. at 5-7.
7Id. at 5.
8Id. at 6.
9Id.
10Id.
11Id.
12Id.
13Id.
14Id. at 7-8.
15Id. at 8.
16Id.
17Id. at 6-7.
18Id. at 8.
19Fed. Bureau of Prisons, Form BP-A0331, Authorization to Receive Package or Property ( June 2010), https://www.bop. gov/PublicInfo/execute/forms?todo=query.
20Fed. Bureau of Prisons Health Servs., National Formulary, Part I 6 (May 16, 2019), https://www.bop.gov/ resources/pdfs/2019_winter_national_formulary_part_I.pdf. 21A list of the approved medications on the BOP Formulary, including the generic equivalents for commonly used brand-name prescriptions, is available on the BOP website at https://www.bop. gov/resources/pdfs/2019_winter_ national_formulary-part_II.pdf.
22Id.
23Fed. Bureau of Prisons Health Servs., supra note 20, at 4-6.
24Id. at 12-32.
25Id. at 2.
26Mental Health Am., Position Statement 56: Mental Health Treatment in Correctional Facilities (Mar. 7, 2015), https://www.mhanational.org/issues/position-statement-56-mental- health-treatment-correctional-facilities#:~:text=Position%20 Statement%2056%3A%20Mental%20Health,Correctional%20Facil- ities%20%7C%20Mental%20Health%20America&text=Mental%20 Health%20America%20understands%20that,in%20all%20that%20 we%20do.
27Allen J. Beck, Use of Restrictive Housing in U.S. Prisons and Jails, 2011-12 6, Bureau of Justice Statistics (Oct. 2015), https:// www.bjs.gov/content/pub/pdf/urhuspj1112.pdf.
34Federal Correctional Complex, Doctoral Psychology Internship, 2018-2019 8, https://www.bop.gov/jobs/docs/ pex_internship_201709.pdf (last visited Jan. 17, 2021); Federal Medical Center, Pre-Doctoral Psychology Internship 2019-2020 5, https://www.bop.gov/jobs/docs/rch internship_
brochure20200904.pdf (last visited Jan. 17, 2021). 35Fed. Bureau of Prisons, supranote30, at6-3. 36Id. at 3-1 through 3-5.
37Fed. Bureau of Prisons, Directory of National Programs 18 (Sept. 13, 2017), https://www.bop.gov/inmates/custody_and_ care/docs20170914_BOP_National_Program_catalog.pdf.
38Id.
39Fed. Bureau of Prisons, supra note 30, at 5-1 through 5-7. 40Fed. Bureau of Prisons, Substance Abuse Treatment, http:// bop.gov/inmates/ custody_and_care/substance_abuse_treatment. jsp (last visited Dec. 15, 2020).
41Id.; 28 C.F.R. § 550.51.
42Fed. Bureau of Prisons, supra note 40.
4328 C.F.R. § 550.52.
44Fed. Bureau of Prisons, supra note 40.
4528 C.F.R. § 550.53(a)(1).
4628 C.F.R. § 550.53(b).
47Id.
48Fed. Bureau of Prisons, supra note 40.
4928 C.F.R. § 550.55.
50Id.
51U.S. Dep’t of Just., Legal Resource Guide to the Federal Bureau of Prisons 29-30 (2019), https://www.bop.gov/ resources/pdfs/legal_guide_march_2019.pdf.
52Id. at 30.
5318 U.S.C. § 4248.
54John Rhodes & Daniel Donovan, Branded for Life by the Modern Scarlet Letters: Do Convicted Sex Offenders Have Rights While on Parole, Probation, or Supervised Release?, 38 The Champion 14, 17
(2014).
55U.S. Dep’t of Just., supra note 51, at 23.
56Id.
5718 U.S.C. § 4322. Exceptions to the prohibition on use of restraints include patients who pose an immediate and credible risk of flight that cannot be prevented by other means, patients who pose an immediate and serious threat of harm to themselves or others that cannot reasonably be prevented by other means, and patients for whom the treating healthcare provider determines that restraints are appropriate for the medical safety of the prisoner.
58Departments of Health, Education, and Welfare Appropriation Act of 1977, Pub. L. 94-439, § 209, 90 Stat. 1418 (1977); see also H.R. Rep.
No. 94-1555 (1976).
59Fed. Bureau of Prisons, Birth Control, Pregnancy, Child Placement and Abortion 3 (Aug. 9, 1996), www.bop.gov/policy/ progstat/6070_005.pdf.
60Id. at 4.
61Fed. Bureau of Prisons, Community Corrections Center Utilization and Transfer Procedures 5 (Dec. 16, 1998), www. bop.gov/policy/progstat/7310_004.pdf.
62Id. at 10-11.
63Id. at 9; Lisa Barrett & Jamila T. Davis, How to Navigate through Federal Prison and Gain an Early Release (2015). 64Barrett & Davis, supra note 63.
65Id.; Zelma W. Henriques & Bridget P. Gladwin, Pregnancy and Motherhood Behind Bars, in Special Needs Offenders in Correctional Institutions (Lior Gideon ed., 2012).
66Fed. Bureau of Prisons, supra note 30, at 4-1 through 4-3. 67Fed. Bureau of Prisons, Education, Training and Leisure Time Program Standards 3-4 (Feb. 18, 2002), https://www.bop. gov/policy/progstat/5300_021.pdf.
Express remorse, while still understanding the victim’s pain, suffering, and how it has impacted them.
Agree with the court as to the seriousness of the crime, without minimizing it. Expand on this topic
What in your life brought you to this moment, what happened that caused you to do this?
What has this experience taught you? Did it bring up moments from your past?
Explain to the Judge that you have a plan (only if you do),
to start making this right with those you have victimized –
or if you have already started, what are they,
no matter how small those efforts have been?
If it’s been a year or so since your verdict, what have you been doing?
(1)Working, (2)volunteering, or watching: (3)TV (only options 1 and 2 are correct).
What is your plan to never re-offend? If there was a “trigger,” what was that trigger, and how do you remove it from your life?
III) COVID, unfortunately, will be with us for a long time, like the seasonal Flu.
Unfortunately, it is much more lethal.
2022/2023, We’ve gone from pandemic to endemic
Practically all that means is that as a society:
Some believe in prevention and others do not
The result is that while influenza has a ~ 52K deaths / per year
COVID and its variants may be 10 x as much
More importantly, new strains are more than likely to present themselves, and masks along with new technology in indoor air filtering are in our future.
Long-COVID, Long-Haulers, or Post-COVID; these symptoms may be mitigating factors to present before the presentence interview as no jail, or prison (state or federal) is equipped to provide the necessary care.
Beyond that, this would not be a qualifier for either 100% CARE LEVEL III or ADL as the symptoms could keep one between sleep, the bathroom, meals, and at best a short walk.

 ensure outside necessary medical care is within close proximity to the designated institution. Care Level III inmates include those needing “companions” to help with their activities of daily living (but not needing daily nursing supervision) and those needing daily to monthly medical or psychiatric visits.
ensure outside necessary medical care is within close proximity to the designated institution. Care Level III inmates include those needing “companions” to help with their activities of daily living (but not needing daily nursing supervision) and those needing daily to monthly medical or psychiatric visits. 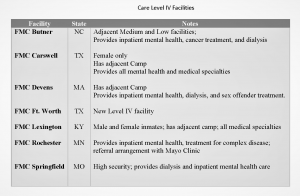 (MCFP) or Federal Medical Centers (FMC). They operate like small hospitals and provide varying degrees of nursing and medical care, including surgical, diagnostic, and therapeutic services. They are the only BOP facilities able to provide Care Level IV inmates with the around-the-clock nursing care needed for acute
(MCFP) or Federal Medical Centers (FMC). They operate like small hospitals and provide varying degrees of nursing and medical care, including surgical, diagnostic, and therapeutic services. They are the only BOP facilities able to provide Care Level IV inmates with the around-the-clock nursing care needed for acute