
TRULINCS EMAIL
The Rules for Email are set in The BOP Program Statement P5265.13. 
- TRULINCS: email Sent From someone in the BOP.
- CORRLINKS: email Received either by persons outside of prison, or with the Warden’s Permission, other inmates in different facilities.
“TRULINCS” is charged based on $0.05/ minute, with the funds removed from your Commissary Account. This includes all of your time “On The System;” no matter whether you are reading a message, typing, or printing (at 0.15 cents per page).
-
- Your maximum time is 30 minutes, and then you must wait another 30 minutes before logging back on if there is a computer free.
- Minutes are sold in lots ranging from 40 to 600.
- Messages can be ~ 2000 words or 13000 characters (and you will see a “countdown timer” in case you lose track).
- Everything is plain text, with no special symbols; nothing fancy.
- There is No Message Forwarding, but you can send a message to multiple persons at one time. If you are found to be forwarding messages, at minimum you may have restrictions put on your usage of the system.
- Printing messages cost 15 cents per page.
- An inmate could be restricted from TRULINCS (the public messaging system) in the following circumstances:
- The person has a history that threatens institutional security or the public.
- A prisoner is under investigation for Disciplinary Violations related to TRULINCS, or Corrlinks abuse or misuse.
- Disciplinary sanctions have restricted the person from emailing for a specific period.
- When there are particular email or sexual offense criminal charges.
CORRLINKS: No forwarding any message to third parties!
USING TRULINCS
- Is considered a privilege; therefore, the Warden or other authorized representative may limit or deny that privilege to any person.
- Individual inmates may be excluded from program participation as part of classification procedures, where the Warden makes the final determination.
- All incoming and outgoing electronic messages, including transactional data, message contents, and other activities, are monitored and retained. [FYI: all that you do is monitored in prison, please don’t try to outsmart them.]
- BOP staff can reject individual messages sent to or from inmates using TRULINCS that jeopardize the institution’s interests.
- Each inmate’ acknowledges, and voluntary consent must be documented on the Inmate Agreement for Participation in TRULINCS Electronic Messaging Program Form (BP-0934).
TRULINCS RESTRICTIONS
- When it is determined that their use would threaten the safety, security, or orderly running of the institution or the protection of the public and staff.
- A Public Safety Factor – Sex Offender, does not automatically exclude them from participation.
- Pending Investigation or Disciplinary Action for Possible Messaging (TRULINCS) Abuse or Misuse. A messaging restriction in this situation is discretionary to ensure the institution’s safety, security, and orderly operation, or the protection of the public and staff.
- Inmates may only exchange electronic messages with persons in the community who have accepted the inmate’s request to communicate.
- Attorneys, “special mail” recipients, or other legal representatives on their electronic message contact list, with the acknowledgment that electronic messages exchanged with such individuals will not be treated as privileged communications and will be subject to monitoring.
- Inmate to Inmate Communication. An inmate may be permitted to correspond via electronic messaging with an inmate confined in any BOP facility if the other inmate is either a member of the immediate family or is a party or witness in a legal action in which both inmates are involved. The following additional limitations apply:
- The appropriate Unit Manager at each institution must approve in writing the correspondence if both inmates are members of the same immediate family or are a party or witness in a legal action in which both inmates are involved.
- The Warden will be informed of any unusual circumstances about a request to correspond electronically for members of the same immediate family or for inmates who are a party or witness in the same legal action.
OUTGOING MAIL LABELS
-
- Ordinarily, inmates are required to place a TRULINCS-generated mailing label on all outgoing postal mail.
ELECTRONIC MESSAGE MONITORING
- Electronic messages sent or received by inmates at all security levels are subject to monitoring for content by trained staff.
TRULINCS Email Contact Request Form BPA1054
-
- This form allows two contacts per page and is very detailed.
- From prison, an email will be sent out.
CORRLINKS: email Received either by persons outside of prison, or with the Warden’s Permission, other inmates in different facilities.
CORRLINKS
- You may or may not receive an email alert, that you have a CORRLINKS
- So if you get to this part first, great.
- As you see, you will need to Register.
- Enter: Your email and create a password.
ON YOUR FIRST CORRLINKS LOGIN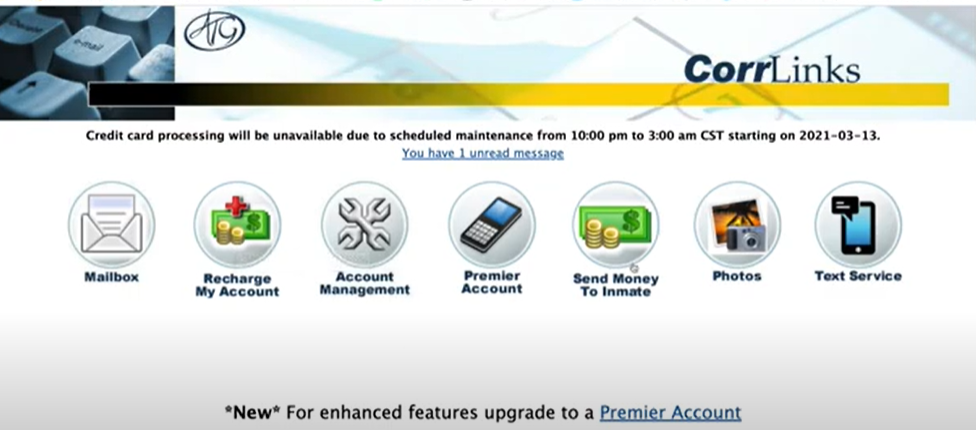
- You will see all of these choices below.
- The only one that I believe we need to work on now is Mailbox.
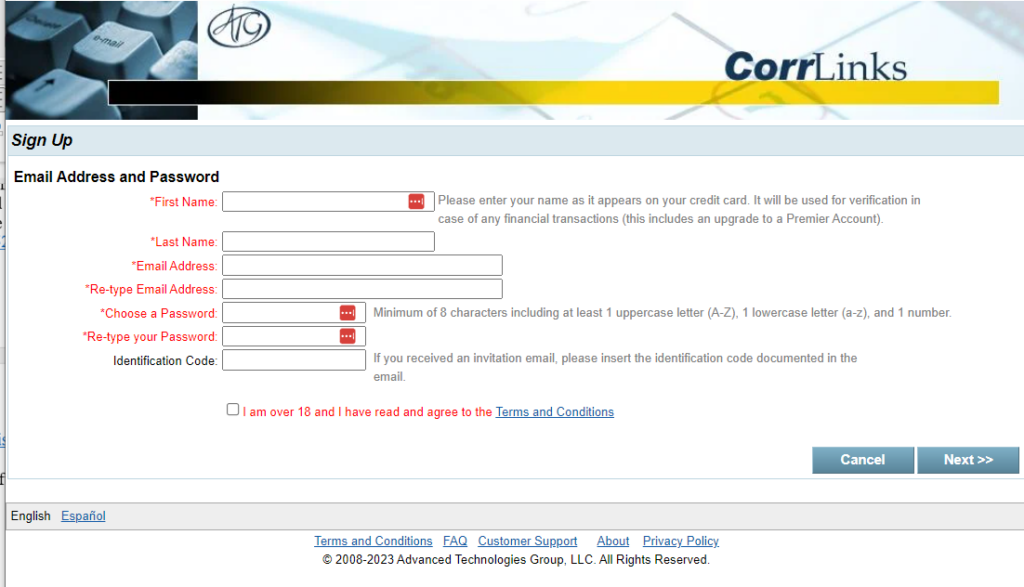
THE REGISTRATION CONTINUES
- It may not be exactly in this order, but fill out all of your information that is in RED.
- You will also see that there is a space for an Identification Code.
- When you get the alert that you have your first email, Do You Accept It?
- If yes, there will be an IDENTIFICATION CODE (which may expire in “10 Days”),
- Copy that code and enter it on Your Registration Form ⇓
YOU NOW CORRESPOND FROM YOUR PC,
YOUR APPLE DEVICE, OR
GOOGLE.
CorrLinks Guide: An Overview
- CorrLinks is a reliable and convenient web-based email system that allows authorized users to communicate with inmates through secure email. To use this service, you need to create an account, purchase credit, and add inmates to your contact list. Once you complete these steps, you can send messages to inmates, who can conveniently receive and respond to them using a secure kiosk within the prison.
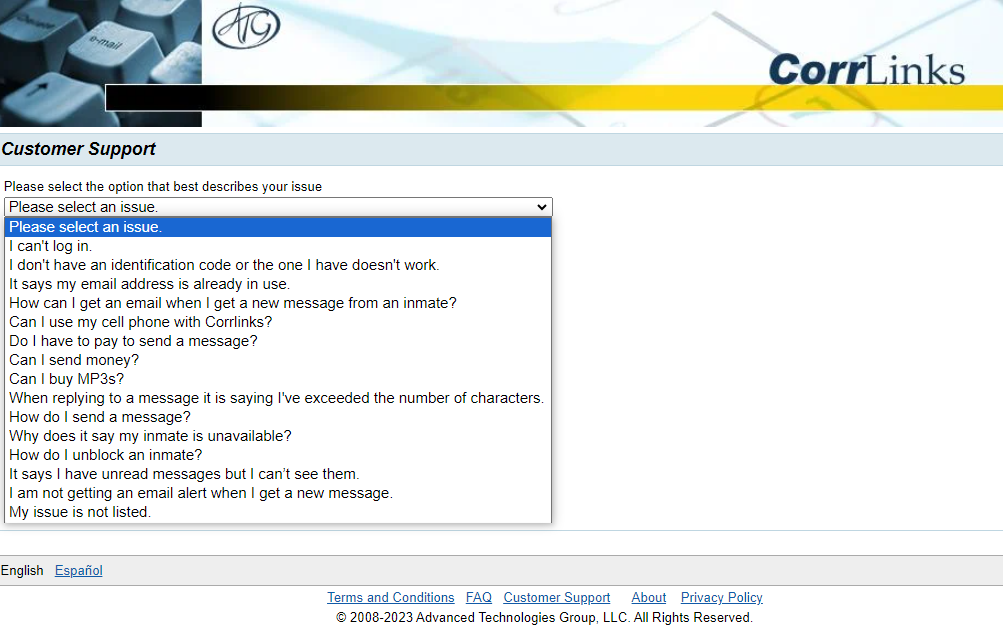
- Forgotten your password on CorrLinks – don’t worry. The system has got you covered! Simply reset your password, it’s a quick and easy process. Please note that CorrLinks won’t be able to personally assist you with this, but rest assured that their system is designed to help you with password resets.
- Your first email alert from your loved one. Upon receiving an alert that an inmate wants to add you to their account on CorrLinks, you simply need to accept the request to begin exchanging messages with them.
- If you’re thinking about blocking an inmate on CorrLinks, it’s important to know that it’s not a decision to be taken lightly. Once you’ve blocked them, it can be difficult to undo the process. You’ll have to go through a lengthy process of sending a written request to the institution to remove the block. It’s important to note that the institution’s mailing address can be found on the Federal Bureau of Prisons website. Once the block is removed, the inmate will have to send you another invitation to add your email again. If you’re certain that you want to block an inmate, you can easily do so by selecting the “block contact from an inmate” option or “block contact from every inmate at a specific facility” option from the menu on CorrLinks. But remember, it’s important to think through your decision before proceeding.
- CORRLINKS Customer Support.
PHONE CALLS
- Inmate Phone Calls Are Recorded and Monitored
- No three-way telephone calls are allowed and this will result in you being disciplined.
- The hours may start as early as 6:00 a.m. and extend as late as 11:30 pm.
- Inmates can make up to 300 minutes of prison phone calls each month, each for 15 minutes.
- In most cases, inmates must wait one hour from the start of their last prison phone call before they can place another call.
- When making a collect call, the recipient must agree to pay for the call.
- $0.06 to $0.38 each minute for local calls and
- $0.56 per minute when calling long distance.
- Direct-dial telephone call costs are subject to change, taken from your commissary account, and are currently as follows:
- Local calls: $0.06/minute
- Long-distance calls in the U.S.: $0.21/minute
- Calls to Canada: $0.35/minute
- Calls to Mexico: $0.55/minute
- Other international calls: $0.99/minute
- In November and December, the prison Warden may authorize an additional 100 minutes, on top of the allowed 300 minutes.
- Biden signs a bill to fight Expensive State Prison phone call costs, JANUARY 6, 2023
- Incarcerated people pay about 5 dollars for a 30-minute phone call. A new bill wants to change that.
CELL PHONES
- The new law makes possession or use of a cell phone or wireless device a crime punishable by up to a year in prison.
- The law also covers the smuggling of cell phones into the BOP.
- Good Time Credits and Earned Time Credits may also be lost, as well as possibly going to The SHU or triggering a change in prison.




 very impressed with lawyers who show legal advocacy in their presentence memorandum ondisputed guideline issues. I appreciate lawyers who give me everything I need well in advance of the hearing.”
very impressed with lawyers who show legal advocacy in their presentence memorandum ondisputed guideline issues. I appreciate lawyers who give me everything I need well in advance of the hearing.”

