Doctor, ‘Patient-Care’ – Out
Non-Medical, ‘Legislator-Care’ – In
Today Families and Their Physicians are faced with impossible choices.
Recently, some states have enacted Legislator Directed Patient Care, that conflict with the doctor-patient ethical relationship, and the oath, to do no harm.
Since forever, as part of that relationship, providers try to educate patients to make decisions for themselves, about what they feel is right for them, says “Dr. Stephanie Mischell.”
- For some doctors, the debate comes down to medical ethics.
- But now, can providers (or anyone) even discuss, refer, or contact out-of-state providers to give them information about patients, regarding abortion services without the fear of litigation, or prosecution?
Prenatal Care.
Prenatal Care may also be affected, particularly if they allow prosecutions to go forward against women.
- Healthcare providers might find themselves caught in the middle – being forced to make ethical choices when asking routine past history questions regarding past pregnancies, and their outcomes.
- In doing so, they may place themselves and their patients in the position of being criminally prosecuted, for what otherwise would have been considered usual and customary medical care.
Heartbeat Detection.
Pediatric cardiologist and researcher, Colin Phoon of New York University Langone Health, shared that before the sixth week, “there is no heart; there’s nothing beating.”
- What they are hearing is “a little flutter in the area that will later become, the future heart“- but
It’s not the actual heartbeat, said another physician, Dr. Saima Aftab, medical director of the Fetal Care Center at Nicklaus Children’s Hospital in Miami.
Erika Werner, a maternal-fetal medicine physician at Brown University, and a Society for Maternal-Fetal Medicine board member explained, “You can see a little flicker,” she said.” That’s it.
As a product manual (Huntleigh High Sensitivity Pocket Dopplers) for one such device explains, the sound is the amplified version of the difference between the transmitted and received signals.
- “It is not the real sound made by blood rushing through an artery or vein, or movement of the fetal heart.”
- It’s only been in the last few decades that doctors have been able to detect this “flutter” at six weeks, thanks to the use of more sophisticated ultrasound technologies.
- …at around 21-23 days after conception, two groups of cells form a horseshoe – known as a heart tube,
- with cells creating a sound that seems like the first heartbeat,
- although it may not pump the blood for another day or two.
All of the major structures appear mostly intact after nine weeks and one day of pregnancy when the entire process is largely complete.
Lupus.
In patients with Lupus (an autoimmune disease), should an inflammatory response flare during their pregnancy, this could then rise to the level of being considered “high risk“.
- In this case, trained medical providers’ treatment plans may be interrupted by Legislator Directed Patient Care, without medical training, forcing themselves into the doctor-patient relationship, which may result in the loss of life. A scary result when considering Dobb’s.
Should the physician decide to ignore Dobbs, and provide what is the standard of care in the medical community, that would likely result in pregnancy loss or miscarriage, they and possibly their patients could expect to be criminally prosecuted – as you see, these are not easy decisions.
- If the moral code of the provider is such that they go ahead and, provide what is considered usual and customary care, that is in line with their medical board code of ethics, and is the standard of care in the community, how will this impact their future should prosecution proceed?
- Will some providers, depending on the severity of the state’s laws, begin to avoid practicing in those states altogether?
- Could they face incarceration as an example to other providers?
- Where does it end?
The Loss of an Experienced Medical Specialty – Who Suffers?
As state Legislator Directed Patient Care laws insert themselves into the physician-patient care model, this may create ethical issues for the provider, and malpractice liabilities for the doctor, hospital, and their associated healthcare systems.
The result of having no contingency plans for the “dead space” that immediately followed Dobbs, created this cascading series of events that result in
- reduced access to specialists – in states where certain procedures are not permitted.
- ultimately to be mostly felt by minority populations,
- with a decrease in new resident training,
- leads to a generation of fewer and “less qualified physicians in this niche specialty,” which makes up Obstetrics and Gynecology.
This new wave of disillusioned providers will not be used to being,
- dictated to by non-medically trained legislators who
- do not have their patient’s best healthcare interests at heart, or based on science, and then
- tell them how to practice medicine.
Some may even face incarceration in some of the more extreme states, and if so – is practicing in those states even worth it?
- Will their colleagues look the other way – or be concerned?
- Likely, as we all have gone to school, before books started being banned, of course, we will be concerned.
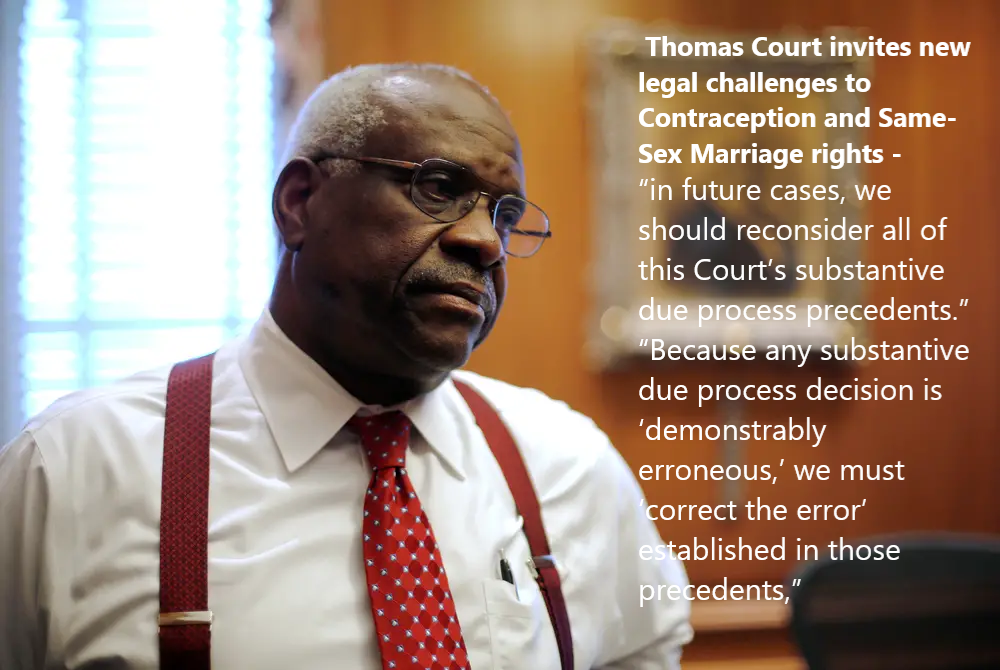
Attorneys | You Can Help The Dam From Breaking | Bloomberg Law |“There is so much confusion”
‘Aiding and Abetting’.
Abortion bans before six weeks in some states depend on enforcement through lawsuits filed by private citizens.
Possible targets: abortion providers and anyone who aids and abets an abortion – after an assumed heartbeat is detected – but which is a “flutter,” only.
Hospitals, Healthcare Systems, Telehealth providers, Pharmacists, Nurses, and Providers are all looking to the legal community for guidance, as confusion reigns from Coast to Coast.
Regulations
The Emergency Medical Treatment and Labor Act obligates all Medicare-participating hospitals with emergency departments to furnish all medical conditions that pose serious jeopardy to health, bodily severe impairment, or serious organ damage.
This duty extends to emergency care for pregnancy or pregnancy loss.
Regarding Catholic Hospitals, the ACLU has collected numerous stories of women being denied emergency care at Catholic hospitals, with more emerging all the time.
Medical Societies Speak Out
By dismantling nearly 50 years of legal precedent, the Court has jeopardized millions of American women’s physical and mental health and undermined the physician-patient relationship’s privacy.
This move will disproportionately impact our most vulnerable populations, such as communities of color, people living in rural areas, and those with low incomes who may have to travel long distances to receive abortions.
Today’s ruling will put many pregnant women and their families into life-threatening and/or traumatic situations.
Unfortunately, with the implementation of Dobbs, doctors have been handicapped in this critical patient-doctor decision-making process. Still, ASCO will work to help our members navigate this new situation and preserve their patients’ access to the highest quality care by providing evidence-based clinical guidance, including fertility preservation, and by advocating for access to all the components of high-quality care.
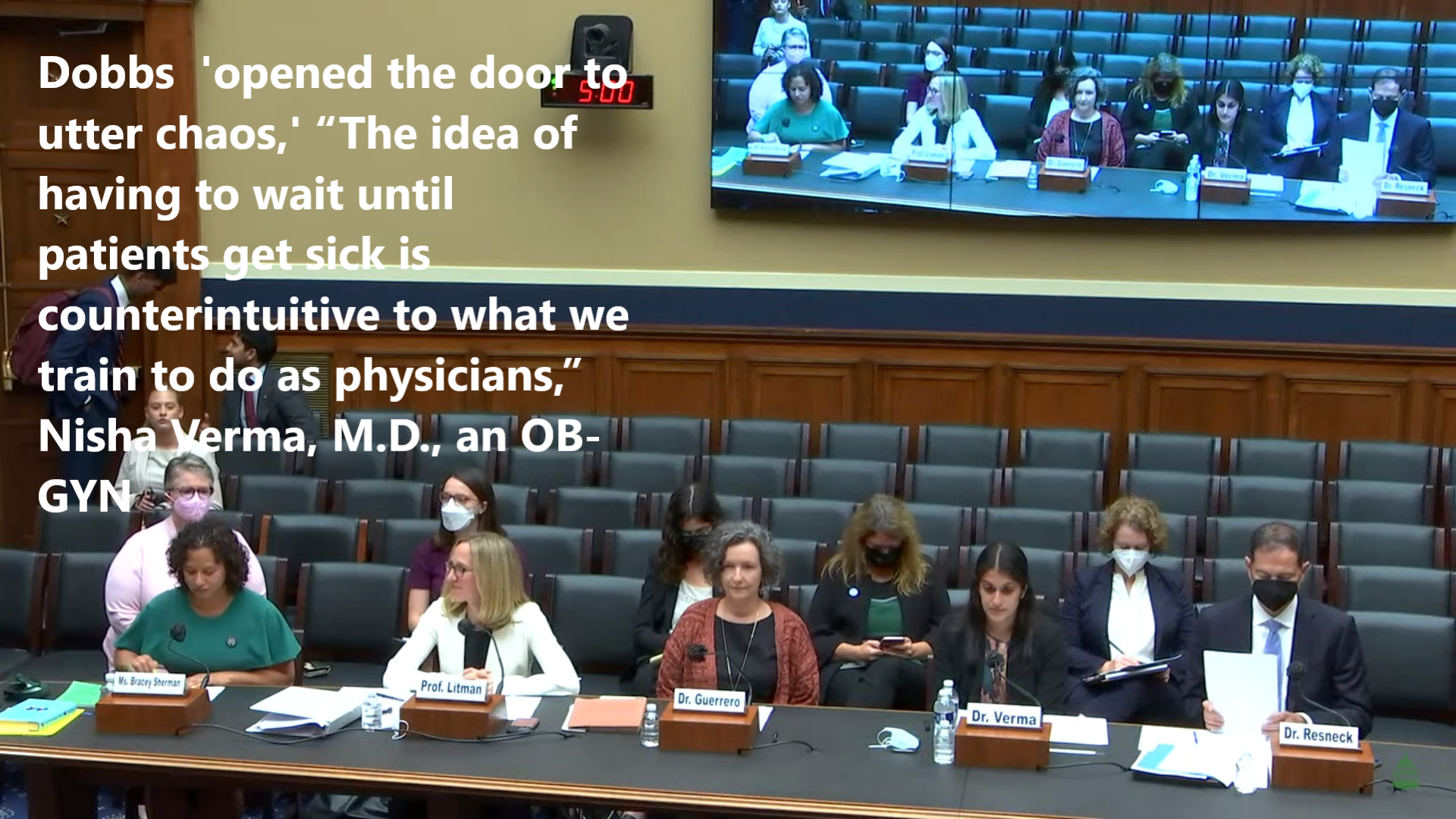
“We are treating this as a disaster response,” Verma said. “We are in an emergency, and this is a disaster.” Its impact on situations will include miscarriage and in vitro fertilization. The practice of medicine will be reshaped, the group said, or even contradicted by “by-laws not founded in science or based on evidence.” She wondered, “Are surgeons going to be afraid to intervene when a pregnant patient ruptures their appendix because they might inadvertently end the pregnancy?”
Today’s ruling means that in many places in the United States, this evidence-based care will be difficult or impossible to access, threatening the health and safety of our patients and jeopardizing the patient-physician relationship.
The Supreme Court’s fig-leaf justification behind these restrictions was that induced abortion was a dangerous procedure that required tighter regulation to protect the health of persons seeking that care. Facts belie this disingenuous rhetoric.1,2. In view of these predictable consequences, the editors of the New England Journal of Medicine strongly condemn the U.S. Supreme Court’s decision
These laws and policies that restrict or otherwise interfere with the patient-physician relationship put patients at risk by limiting access to quality, evidence-based care.






 I- Schizophrenia
I- Schizophrenia could be true, but isn’t; such as being followed, being plotted against, or having a delusion. The delusion lasts for at least 1 month. Symptoms may include;
could be true, but isn’t; such as being followed, being plotted against, or having a delusion. The delusion lasts for at least 1 month. Symptoms may include;
 This condition is caused by the use of or withdrawal from drugs, such as hallucinogens or crack cocaine that causes hallucinations, delusions, or confused speech.
This condition is caused by the use of or withdrawal from drugs, such as hallucinogens or crack cocaine that causes hallucinations, delusions, or confused speech.
